- For Patients
- Introduction to the Marshall Protocol
- Length of the MP
- Immunopathology
- Managing immunopathology
- Food and drink
- Light restriction
- Vitamin D metabolite calculator - get feedback on vitamin D results
- Therapeutic probe - best method for determining MP suitability
- Starting the Marshall Protocol
- Resources for patients
- Marshall Protocol summary
- Palliative vs. curative treatments
- Patient interviews on Bacteriality
- Non-MP treatments
- Glossary
- The Protocol
- Marshall Protocol summary
- Publications and presentations
- Science behind immunopathology
- Science behind olmesartan (Benicar)
- Safety of olmesartan
- Resources for physicians
- Vitamin D metabolite calculator - get feedback on vitamin D results
- Therapeutic probe - best method for determining MP suitability
- Physicians' concerns about the MP
- Notice for emergency medical personnel

- The Pathogenesis
- Publications and presentations
- Science behind Marshall Pathogenesis
- Microbes in the human body
- Successive infection and variability in disease
- Autoimmune theory of disease
- Science behind vitamin D
- Metabolism of vitamin D and the VDR
- Th1 Spectrum Disorder - how chronic inflammatory diseases are related
- Transmission of bacteria and onset of chronic disease
- Evolutionary perspective on disease
- Incidence and prevalence of disease
- Evidence that chronic disease is caused by pathogens
- Diseases
- Foundation
- Related Sites


This is an old revision of the document!
Table of Contents
Health Maintenance and Olmesartan
Summary of research on aging and OlmesartanMedication taken regularly by patients on the Marshall Protocol for its ability to activate the Vitamin D Receptor. Also known by the trade name Benicar. taken from article Science behind olmesartan
with additional studies
Although uncontrolled confounding might still exist, (this was a short term study) olmesartan does not seem to increase cardiovascular risk compared with losartan. 1)
The ROADMAP study will answer the question whether an ARBA drug which is an angiotensin receptor blocker. One of the ARBs is olmesartan (Benicar). Not all ARBs activate the Vitamin D Receptor. can prevent or delay the onset of microalbuminuria and whether this translates into protection against cardiovascular events and renal disease. 2)
Benefits of RAS blockade with olmesartan treatment are sustained after study discontinued. 3)
Data demonstrate potential benefits of reducing the heart rate of type 2 diabetes patients, and indicate that olmesartan could, in particular, reduce the risk of microalbuminuria in patients with low heart rate. 4)
Administration of olmesartan suppressed the accumulation of macrophages in brachiocephalic atherosclerotic plaque. (in mice) 5)
Olmesartan significantly reduced myocardial infarct size and improved LV contractility at a dose (3 mg/kg) with systemic vasodilating effects but not at a lower dose (0.3 mg/kg) without hemodynamic effects.(in rat)
Olmesartan medoxomil reverses left ventricle hypertrophy and reduces inflammatory cytokineAny of various protein molecules secreted by cells of the immune system that serve to regulate the immune system. IL-6 in the renovascular hypertensive rats. 6)
Replacing candesartan with olmesartan decreased LVMI in association with a sustained decrease of plasma Ang II over a 12-month period without changing blood pressure or plasma aldosterone in patients with essential hypertension. 7)
Inhibition of renin-angiotensin system attenuates periadventitial inflammationThe complex biological response of vascular tissues to harmful stimuli such as pathogens or damaged cells. It is a protective attempt by the organism to remove the injurious stimuli as well as initiate the healing process for the tissue. and reduces atherosclerotic lesion formation. 8)
Therapeutic and supratherapeutic OLM doses had no clinically significant effect on cardiac repolarization and were well tolerated. 9)
In conclusion, there is no robust signal for harm with olmesartan use. 10)
General research on aging
Holistic vitamin D supplementation with or without calcium is unlikely to be an effective primary prevention strategy for falls or fracture. There has also been high-quality evidence that vitamin D, daily or as a bolus, does not reduce the risk of cardiovascular events. 11)
When using off-label Olmesartan, patients are observed to need fewer other pharmaceutical preparations to maintain and improve health status. Falls studies have determined that taking ≥ 4 drugs is associated with an increased incidence of falls, recurrent falls, and injurious falls. 12)
Some of the documented protective effects of ARBs
include the ability to:
- inhibit liver fibrosis and aid liver healing15)
- reduce insulin resistance in rats16)
- 6 mg/kg olmesartan reduces the inflammatory process and bone loss in rats17)
- protect the mitochondria from age-associated damage from oxidation18)
- play a protective role against proliferative diabetic retinopathy 19)
- reduce liver fibrosis20)
Olmesartan and other ARBs have been used
to block various bad effects of Angiotensin II, including heart failure. In this regard, olmesartan has been shown to:
- protect the heart from damage from inflammation in myocarditis25)
- ameliorate acute experimental autoimmuneA condition or disease thought to arise from an overactive immune response of the body against substances and tissues normally present in the body myocarditis, in rats, suppressing cytotoxic myocardial injury 26)
- prevent acute left ventricular dysfunction27)
- lower C-reactive protein, one of the acute phase proteins that increase during systemic inflammation28)
- act as an antiarrhythmic29)
- block the production of Angiotensin II, thus improving mortality rates in heart failure patients30)
- This study demonstrated that olmesartan reduced angiotensin II and aldosterone levels more effectively than azilsartan, resulting in a stable antihypertensive effect. Olmesartan also had an inhibitory effect on cardiac hypertrophy. Accordingly, it may be effective for patients with increased RAAS activity after cardiac surgery or patients with severe cardiac hypertrophy. 31)
Dosage
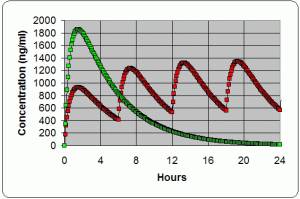
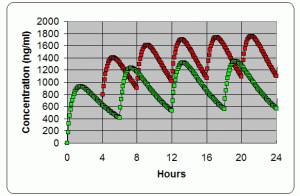
In August 2002, Trevor Marshall and Frances Marshall published a NetPrint about valsartan (Diovan), in which they reported that the once daily dosing of the ARB caused psychedelic dreams and psychotic events in two sarcoidosis patients. On the theory that these symptoms were caused by changes in plasma concentration, the frequency of the dosing of ARB was increased, which ended up reducing symptoms of disease including psychedelic dreams. This early insight into ARBs anti-inflammatory effects led Marshall to conclude that for an ARB to provide symptomatic relief, it was necessary to use more frequent dosing than typical. Professor Marshall would later go on to recommend frequent dosing of another ARB, olmesartan.
In rats, Olmesartan at 6 mg/kg optimally reduced the inflammatory process and bone loss34). That would be 9-10 tablets of Olmetec daily for a 64 Kg human
Olmesartan has also been shown to
A number of studies have found
that olmesartan possesses various ways of protecting the kidneys from the effects of inflammation and cytokine damage:
- in circadian rhythms between HR and MAP in CKD: Synchronization between the two rhythms was progressively lost as renal function deteriorated, and Olmesartan partly restored the synchronization 40)
- in hypertensive patients with CKD, olmesartan add-on therapy improves the ambulatory BP profile via a preferential reduction in nighttime BP with concomitant renal injury inhibition 41)
- results suggest olmesartan can help decrease plasma AGE levels in patients on Hemodialysis 42)
- renal protective effects of olmesartan may be better than those of other ARBs 43)
- olmesartan may uniquely increase urinary ACE2 level, which could offer additional renoprotective effects 44)
Studies also showed
- treatment with olmesartan inhibited bone loss 45)
- olmesartan protects endothelial cells against oxidative stress-mediated cellular injury 46)
- decreases viability of malignant cell lines47)
- carotid IMT and BP decreased similarly with olmesartan and atenolol; but only olmesartan reduced the volume of larger atherosclerotic plaques 48)
- improvement of Plasma Biomarkers after switching stroke patients from other Angiotensin II Type I Receptor Blockers to Olmesartan 49)
- improvement of glycemic control & insulin resistance was only observed in olmesartan group 50)
- OLM substantially delayed the development of left ventricular remodeling in type 2 diabetes 51)
- prevention of microalbuminuria in patients with type 2 diabetes and hypertension 52)
Long term treatment
Patients receiving the highest dose of olmesartan (40 and 80 mg) had an inward carotid remodeling and were shifted toward a lower elastic modulus at a given circumferential wall stress, indicating an improvement in the intrinsic elastic properties of the carotid artery wall material. These data suggest that 40 and 80 mg olmesartan were able to significantly remodel and destiffen the arterial wall material during long-term treatment, partly independently of blood pressure, compared with 20 mg.
hyper.ahajournals.org/content/early/2014/07/07/HYPERTENSIONAHA.114.03282.reprint 53)